Change of Law: Hospital Action Required
| To: | Chief Executive Officers, Chief Financial Officers, Chief Information Officers, Chief Quality Officers, Legal Counsel, and Government Affairs Staff
Please forward to community benefit program managers as well as other impacted staff |
| From: | Ashlen Strong, JD, MPH, Senior Policy Director, Government Affairs AshlenS@wsha.org | (206) 216-2550 |
| Subject: | Hospital Transparency and Reporting (2021 Session E2SHB 1272) |
Purpose
This bulletin informs hospitals about a hospital transparency and reporting law passed in the 2021 Washington State legislative session. Engrossed Second Substitute House Bill 1272 (E2SHB 1272) includes new hospital data collection and reporting requirements in the following areas:
- Detailed hospital financial reporting requirements (expenses, revenues, pandemic funds) effective 1/1/2023
- Consolidated reporting on non-hospital entities owned by hospitals effective 7/1/2022
- Hospital patient demographic data in discharge reporting (Comprehensive Hospital Abstract Reporting System – CHARS) effective 1/1/2023
- Community health improvement services effective 7/1/2022 and community health needs assessments effective 7/25/2021
- Hospital charity care information effective 1/1/2023
The new law also includes a study on the acute care hospital workforce to be conducted by the University of Washington and expands the definition of provider-based clinic. WSHA provided extensive input into the drafting of the bill, including proposing many changes – some were included by the legislature and others were not. We recognize this new law contains several onerous changes to the operational processes for data collection and financial and community benefit reporting for hospitals.
Applicability/Scope
Most elements of this bill apply to all acute care hospitals licensed under chapter 70.41 RCW and behavioral health hospitals licensed under chapter 71.12 RCW. The provision relating to consolidated financial reporting on non-hospital entities (Section 2) only applies to acute care hospitals licensed under chapter 70.41 RCW. The provisions on community health improvement services, community health needs assessments, and charity care information (Section 5) only apply to 501(c)(3) tax-exempt non-profit hospitals. Additionally, WSHA successfully negotiated some relief for critical access hospitals and sole community hospitals, as outlined in the Overview below.
Recommendation
- Review this bulletin and E2SHB 1272 to understand the new requirements. WSHA cannot offer legal advice to members and recommends hospitals engage legal, risk, compliance, and leadership as appropriate to evaluate compliance with the new law.
- Evaluate current hospital standards, policies, and procedures relevant to data collection and reporting with regard to financials, patient demographics, and community health improvement services.
- Participate in WSHA’s member activities on Department of Health rulemaking and other stakeholder engagement, which will take place over the next year.
Overview
While WSHA engaged in negotiations to significantly mitigate the impact of the legislation, this new law requires substantial changes for hospitals. Details of each of the major elements of the new law follow.
I. Detailed Financial Reporting Requirements
Uniform Reporting System Updates
E2SHB 1272 requires the Department of Health (DOH) to revise the uniform reporting system to require additional detail in the “other direct expense” and “other operating revenue” categories of the required hospital expense and revenue reports. DOH must revise these requirements through rulemaking by January 1, 2023.
The new DOH rules will require hospitals to report additional detail on “other direct expenses” and “other operating revenue” for line items and amounts meeting the following criteria:
- Hospitals that are not critical access hospitals or sole community hospitals must report all expenses and revenues that either (1) have a value of $1,000,000 or more or (2) represent 1% or more of total expenses or revenues;
- Critical access hospitals and sole community hospitals must report the greater of expenses and revenues that (1) have a value of $1,000,000 or (2) represent 1% or more of total expenses or revenues.
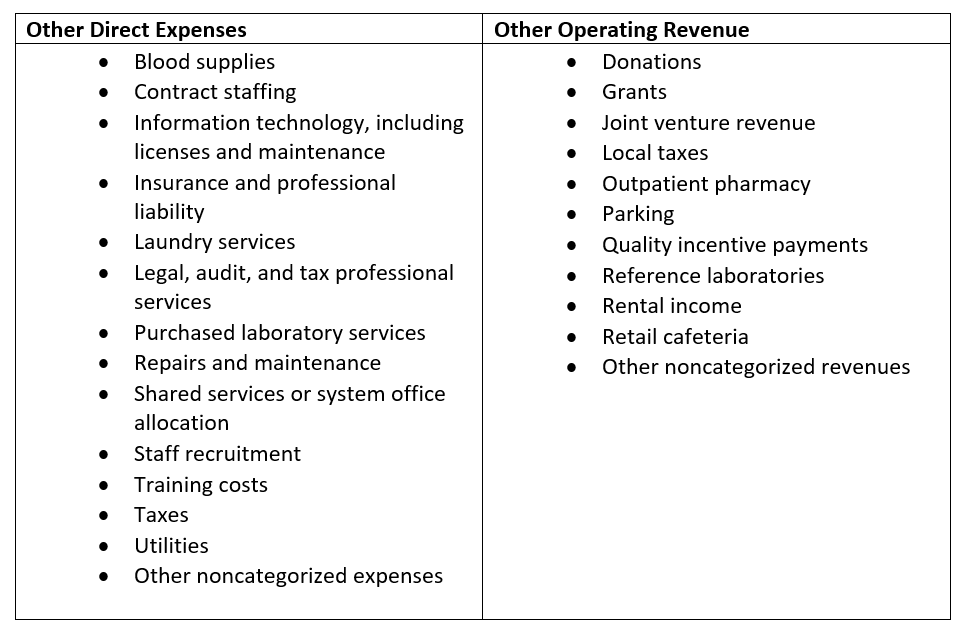
The new law expressly requires DOH to include the additional categories of expenses and revenue outlined in the table below in the Washington State Department of Health Accounting and Reporting Manual and Year-end Reporting Template. Updates to the manual and reporting template require a formal rulemaking process, which DOH intends to begin in early 2022.
Emergency Funds Received from Governments
The new law also requires hospitals to report any money, including loans, received from a federal, state, or local government entity in response to a national or state-declared emergency, including a pandemic. There is also a specific requirement to report any funds received in association with COVID-19 after January 1, 2020. DOH is required to provide guidance to hospitals on how to report this information.
II. Consolidated Reporting on Non-Hospital Entities Owned by Hospitals
Beginning July 1, 2022, all health systems operating a hospital licensed under chapter 70.41 RCW, must annually submit to DOH a consolidated annual income statement and balance sheet that includes all the hospital and non-hospital health care entities it operates in Washington State, including:
- Hospitals
- Ambulatory surgical facilities
- Health clinics
- Urgent care clinics
- Physician groups
- Health-related laboratories
- Long-term care facilities
- Home health agencies
- Dialysis facilities
- Ambulance services
- Behavioral health settings
- Virtual care entities that are operated in Washington
However, public hospital districts that own or operate a hospital are not required to submit the above information and may instead rely on the audited financial statements submitted to the state auditor’s office.
III. Hospital Patient Demographic Data in Discharge Reporting (CHARS)
E2SHB 1272 also requires DOH to develop rules requiring hospitals to gather and report additional patient demographic information by July 1, 2022. These data will be reported via CHARS. Under these rules, hospitals will be required to identify patients by:
- Race
- Ethnicity
- Gender identity
- Sexual orientation
- Preferred language
- Any disability
- Zip code of primary residence
Hospitals will also be required to notify patients that disclosure of this information is voluntary.
The agency will further define these categories and a patient notification process through the rulemaking process. Recognizing the immense burden these changes will place on hospitals, WSHA negotiated a long rulemaking and implementation timeline for this part of the new law. WSHA is actively engaged in the DOH rulemaking process, which is in its early stages and will continue throughout 2022. More information about WSHA member engagement in the rulemaking process is included below under Next Steps.
WSHA negotiated an additional six months between rule adoption (July 1, 2022) and implementation (January 1, 2023) to allow hospitals time to develop policies, procedures, and infrastructure to comply with the new DOH rules.
Connection to Notifiable Conditions Rule
Note that the Board of Health is separately developing new rules about patient demographic information to be collected and reported on notifiable conditions (WAC 246-101-011). This rule only includes expanded race, ethnicity, and preferred language categories.
- Ethnicity: Patients can identify as (a) Hispanic, Latino/a, Latinx or (b) Non-Hispanic, Latino/a, Latinx.
- Race: Patients may choose from a list of 72 different race options. Most reporting entities are currently collecting seven broad race categories. The current categories are American Indian/Alaska Native, Asian, Black/African American, Native Hawaiian/Other Pacific Islander, White, Other, and Unknown. However, the regulations expand the current categories into more detailed identities. For example, the Alaska Native/American Indian race option is broken down into separate Alaska Native and American Indian options.
- Language: Patients may choose from a list of 50 language options
The notifiable conditions rule was originally slated to take effect January 31, 2022, but the Board of Health voted to delay implementation to January 1, 2023 to align with the demographic data collection and reporting requirements in E2SHB 1272. Consideration of whether hospitals prefer the fields in the two data collection and reporting requirements to mirror each other will likely be part of the conversation during agency rulemaking. Learn more in WSHA’s November 18, 2021 bulletin on the notifiable conditions regulation.
Waiver Opportunity for CAHs, Sole Community, and Medicare Dependent Hospitals
Due to WSHA’s advocacy, DOH must develop a waiver process for critical access hospitals (CAHs), sole community hospitals, and hospitals that qualify as a Medicare dependent hospital. WSHA advocated for this provision to allow small hospitals grappling with outdated electronic health record (EHR) systems additional time to come into compliance with the requirements of E2SHB 1272. Hospitals may apply for a waiver due to economic hardship, technological limitations that are not reasonably in the control of the hospital, or other exceptional circumstances demonstrated by the hospital.
The waivers are temporary and must be limited by the agency to a maximum of one year, or for any other timeframe specified by DOH, and hospitals must be allowed to apply for waiver extensions. Development of the details of the waiver program was delegated to DOH and will be part of the agency rulemaking process.
Grant Availability for CAHs, Sole Community, and Medicare Dependent Hospitals
DOH must also develop a grant program for CAHs, sole community hospitals, and hospitals that qualify as Medicare dependent to assist with the costs of updating electronic health record systems to comply with the demographic information collection requirements. The Legislature appropriated $3.7 million to DOH to implement this bill over the course of the 2021-2023 biennium. A portion of that funding goes toward this grant program. Hospitals that are part of a health system are not eligible for the grant program. The grant program must be established by October 1, 2022 and must:
- Consider information about the hospital’s need for financial support to alter the hospital’s electronic health records system, including, but not limited to, demonstrated costs necessary to update the hospital’s current electronic health record system to comply with the requirements in this section and evidence of need for financial assistance;
- Require hospitals that receive grants to update their EHRs to comply with these requirements before updating the EHR for other reasons (other than for security, compliance, or privacy purposes); and
- Require hospitals that receive grants to comply with the demographic reporting requirements by July 1, 2023. Thus, hospitals that receive a grant also receive an additional six months to comply with the demographic data reporting requirements.
IV. Community Health Needs Assessments and Community Health Improvement Services
Community Health Needs Assessment State Reporting
501(c)(3) tax-exempt non-profit hospitals are subject to 501(r) and required by the Internal Revenue Service (IRS) to develop community health needs assessments (CHNAs) every three years. Under current law, hospitals must make CHNAs “widely available,” such as by posting on their websites. E2SHB 1272 adds a new requirement that these hospitals submit their CHNAs to DOH within fifteen days of submission to the IRS beginning July 25, 2021. Hospitals do not have to submit CHNAs completed before July 25, 2021 and will continue to follow their current three-year cycles with the IRS. The law also requires DOH to post all submitted hospital CHNAs on its website; the agency has not yet identified a webpage for this information.
According to E2SHB 1272, Section 5(2)(a), if not already included in the CHNA, hospitals subject to this requirement will also be required to submit “a description of the community served by the hospital, including both a geographic description and a description of the general population served by the hospital; and demographic information such as leading causes of death, levels of chronic illness, and descriptions of the medically underserved, low-income, and minority, or chronically ill populations in the community.”
New Community Health Improvement Services Addendum
Beginning July 1, 2022, 501(c)(3) tax-exempt non-profit hospitals will also be required to complete a CHNA addendum including more detailed information about “community health improvement services” and submit the addendum to DOH on an annual basis. The law does not define “community health improvement services,” nor refer to any other legal definition. However, because the new law refers to hospitals required by the IRS to complete CHNAs, it would be reasonable to infer the intent was to reference the definition used in the IRS 990 Form H.
The 2020 Instructions for IRS 990 Form H define “community health improvement services” as:
“Community health improvement services” means activities or programs, subsidized by the health care organization, carried out or supported for the express purpose of improving community health. Such services don’t generate inpatient or outpatient revenue, although there may be a nominal patient fee or sliding scale fee for these services. (Page 16)
The instructions continue to explain that community need for an activity or program must be established and can be demonstrated through a CHNA, a request from a public health agency or community group, or involvement of community benefit organizations unrelated to the hospital. (Page 16)
The instructions then include this guidance: “Community benefit activities or programs also seek to achieve a community benefit objective, including improving access to health services, enhancing public health, advancing increased general knowledge, and relief of a government burden to improve health.” (Page 16)
In summary, the IRS definition of “community health improvement services” is quite broad and includes a wide variety of programs and activities designed to improve community health, whether provided directly by the hospital or supported through investment.
DOH is required to develop a standardized form for the addendum and to post the information it collects on its website. The addendum will include the following elements:
- Type of activity;
- Method in which it was delivered;
- How it related to an identified community need in the CHNA;
- Target population for the activity;
- Strategies to reach the target population;
- Identified outcome metrics;
- Cost to the hospital to provide the activity;
- Methodology used to calculate the hospital’s costs;
- Number of people served by the activity; and
- If the activity is performed by an entity other than the hospital, the name of the entity.
CHIS Addendum Reporting Threshold
Non-profit hospitals that are not critical access hospitals or sole community hospitals will be required to submit an addendum that details community health improvement services with a cost of $5,000 or more.
Non-profit critical access hospitals and sole community hospitals must submit an addendum that details information about the ten highest cost activities identified as community health improvement services.
Demographic Reporting of Participants in CHIS
The addendum will also require hospitals to document demographic information about “participants” in community health improvement services, including:
- Race
- Ethnicity
- Any disability
- Gender identity
- Preferred language
- Zip code of primary residence
DOH may revise the demographic information collected according to a six-year review cycle.
“Participant” is not defined in the new law, but this is likely to include the beneficiaries of community health improvement services, such as those attending a health fair, receiving a free mammogram, or playing in a community playground funded by the hospital. Hospitals will be required to inform participants in community health improvement services that disclosure of their demographic information is voluntary. Depending on the definition of “participant,” some participants will be more challenging to identify for data collection and notification purposes.
Under the new law, DOH is required to consult with community organizations that provide community health improvement services, communities impacted by health inequities, health care workers, hospitals, and the governor’s interagency coordinating council on health disparities in developing guidelines around collection of demographic information. The definition of “participant” and the process for informing them of the voluntary nature of disclosure of demographic data are examples of details that may be addressed in the DOH stakeholder engagement process. Read more about the DOH stakeholder engagement process under Next Steps.
V. Hospital Charity Care Reporting
Beginning January 1, 2023, every hospital will be required to report to DOH, on a quarterly basis, the number of submitted and completed charity care applications received in the prior quarter and the number of approved charity care applications in the prior quarter. DOH must develop a standard form for hospitals to use in submitting this information. WSHA will work closely with DOH and stakeholders in the development of this standard form and reporting process.
Acute Care Hospital Workforce Study
In addition to the hospital financial and demographic data reporting changes outlined above, E2SHB 1272 also requires DOH to study hospital workforce. This study is unrelated to the changes in hospital data collection and reporting requirements. It requires DOH to “contract with the University of Washington school of nursing to lead an interdisciplinary study to analyze the impact of the number, type, education, training, and experience of acute care hospital staffing personnel on patient mortality and patient outcomes utilizing scientifically sound research methods most effective for all involved stakeholders.” The study must be completed by September 1, 2022 and a report submitted to the Legislature by October 1, 2022.
Next Steps
In June 2021, DOH released its first notice of intended rulemaking related to this bill for the section on demographic information to be collected upon discharge (CHARS). WSHA is following this closely and will participate in the rulemaking process.
Additionally, WSHA is creating three workgroups of hospital members to inform our comments on three broad topics covered in E2SHB 1272:
- Financial Reporting
- Demographic Information Reported Upon Discharge
- Community Health Improvement Services Reporting
While the language in the new law cannot be altered without further legislative action, the administrative rulemaking process provides us with important opportunities to influence the way the new law is implemented. We look forward to learning more about our members’ thoughts on the way DOH should administer these new requirements and how WSHA should advocate to DOH.
WSHA’s 2021 New Law Implementation Guide
Please visit WSHA’s new law implementation guide online. The Government Affairs team is hard at work preparing resources and information on the high priority bills that passed in 2021 to help members implement the new laws, as well as links to resources such as this bulletin. In addition, you will find the Government Affairs team’s schedule for release of upcoming resources on other laws and additional resources for implementation.
Background and References
- Engrossed Second Substitute House Bill 1272 (E2SHB 1272)
- DOH Preproposal Statement of Inquiry (WSR 21-13-095)


