Ensuring patients receive treatment in their language of care (LOC) improves outcomes, reduces disparities and quickens the process of getting care in life-threatening situations. This report examines the geographic distribution of LOC in Washington state and identifies health care disparities by LOC via visualizations of sepsis mortality.
This report also reveals regional demands for specific languages, underscoring potential inequities within limited-resource areas, implications for healthcare access, and the critical need for interpreters and culturally tailored care strategies to ensure more equitable health care delivery. We encourage readers to stratify their equity analyses by language and further investigate LOC disparities with clinical teams.
Background
Washington is a state with well-established and ever-expanding linguistic diversity. Increasing immigration has shaped Washington’s linguistic landscape, as Washington saw a 29% increase in its immigrant population from 2010-21.1 We also continuously rank as one of the top ten resettlement states in the U.S., welcoming over 30,000 refugees from more than 70 countries in the past decade.2 Consequently, 21.5% of people five years and older in 2023 spoke a language other than English at home, of which 36.6% spoke English less than “very well.”3
In a hospital environment designed for a predominantly English-speaking population, this language barrier can pose significant risks to patient safety. Previous studies have linked language barriers to worse health outcomes, including higher rates of serious medical events,4,5 longer hospital stays,6 higher readmission rates,7 misdiagnosis,8 delayed treatment5,9,10 and higher mortality rates.11
We echo these conclusions on the importance of LOC in healthcare delivery and outcomes by including a stratified analysis of sepsis mortality by LOC. Sepsis, a life-threatening organ dysfunction caused by a dysregulated response to infection, is the leading cause of hospital mortality, constituting an estimated 30-50% of hospitalizations culminating in death.12 Sepsis is also the most expensive condition to treat in the U.S. healthcare system.13 As such, identifying and addressing language barriers in sepsis care is crucial for improving patient outcomes and reducing healthcare costs.
Summary of Findings
Geographic Distribution of Language

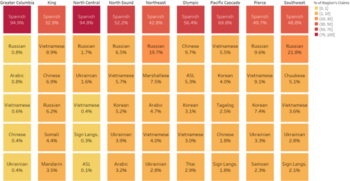
The Washington State Discharge Dataset collects data on patients’ self-reported LOC. Figure 2 outlines the distribution of the most spoken languages other than English in the dataset across Washington State Healthcare Authority’s Accountable Communities of Health (ACH) regions, whose boundaries are outlined in Figure 1. ACHs serve the Washington state Medicaid population using community-based care coordination strategies; delineating by their regional boundaries can help inform hospitals of the varied language needs of patients who access their facilities.
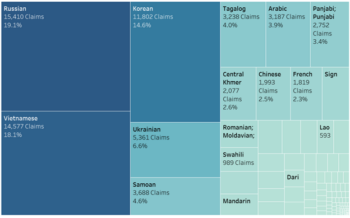
Figure 2 outlines an important concept: language needs in Washington are regionally distinct, forming unique pockets of demand. Spanish speakers comprise a larger percentage of non-English LOC reports in rural regions compared to more urban regions of Washington. In contrast, East Asian languages, such as Vietnamese, Chinese, and Korean, comprise a higher percentage of non-English speakers within urban regions. High rates of Eastern European LOC claims, including Ukrainian and Russian, can also be found within specific pockets of the state (see Figure 3 for the Pierce ACH Region below). Thus, hospitals designing their language access plans should consider the specific language needs of their patients, as well as the growing and emerging language needs within the regions they serve over time.
Concurrently, the geographic distribution of Figure 2 shows that rare-language speakers (e.g. Marshallese, Chuukese) often reside within rural regions. Rural communities have less resources available compared to urban centers, compounding challenges in providing equitable care and requiring hospitals to think creatively about collaboration to address rare language access within their region.
Sepsis Mortality by Language
Ensuring hospital services are delivered with the assistance of a qualified medical interpreter, or in a patient’s language, is essential for ensuring quality of care. This is particularly important for emergency departments, where there is little to no lead time and life-threatening conditions must be treated promptly. For example, timely identification of sepsis is essential to reducing mortality.14 Language barriers may delay diagnosis and the initiation of sepsis bundles. Using DASH Premium, we explore sepsis mortality by LOC, as defined by WSHA.1
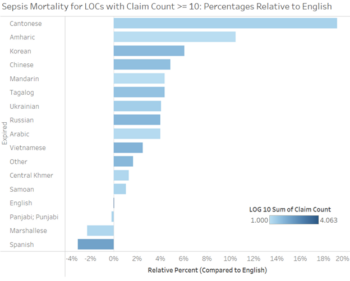
With English as a reference group, we notice broad variation in sepsis mortality rates. In Figure 4, sepsis mortality is shown, per language, relative to English speakers.
From this, we see that discharge outcomes for sepsis patients vary significantly by language of care. For example, ten percent more Amharic speakers died compared to English speakers due to sepsis from 2022-24. Raising staff awareness of similar outcome disparities by language, training them to identify language needs and providing guidance on establishing access to remote interpreter services will help ensure timely sepsis diagnosis and treatment.
As with stroke and heart attack, timely diagnosis of sepsis is paramount. With as many as 87% of sepsis cases originating in the community,15 not in hospitals, it is essential to provide educational resources on sepsis symptoms in the appropriate language. This highlights a critical opportunity to inform patients about sepsis—in their LOC—at the point of hospital discharge, in clinical settings and at hospital health fairs or events.
Conclusion
This analysis underscores the importance of including language of care in explorations of healthcare delivery and outcomes in Washington State hospitals. By understanding how language barriers lead to inequities, healthcare providers and policymakers can take critical steps towards ensuring all patients receive safe, effective and equitable care. For example, hospitals can refer patients to the Parent Support Warm Line (1-888-404-PPMD (7763)) or the general Washington Warm Line (1-877-500-9276), operated by bi-lingual/bi-cultural Spanish speaking staff with interpreter services available for patient speaking languages other than English and Spanish. The line provides emotional support, education wellness and self-care planning.
For questions on this analysis, reach out to Lindsey Sydnor at lindseys@wsha.org. For more dashboards and ad-hoc explorers, please visit the DASH and DASH Premium website. If you have any questions or want to learn more, please contact Ed Phippen edp@wsha.org and datanalytics@wsha.org.
Limitations
This analysis is limited to claims information and demographic reporting required by the state within the years 2022 to 2024. To accurately identify the drivers of healthcare inequities, additional data is required, including qualitative information from frontline staff. Additionally, data is not available to show when an interpreter was requested and if the request was filled. Lastly, claims data is limited to the correct reporting of language of care, which may not be accurate in all cases.
___________________________
1Wei Yen (2023, May). Washington state’s immigrant population: 2010-21. OFM Health Care Research Center Research brief No. 110. https://ofm.wa.gov/sites/default/files/public/dataresearch/researchbriefs/brief110.pdf.
2Washington State Department of Social and Health Services. (n.d.). Refugee Resettlement. https://www.dshs.wa.gov/esa/csd-office-refugee-and-immigration-assistance/refugee-resettlement.
3United States Census Bureau (2023). American Community Survey S1601 | Languages Spoken at Home. https://data.census.gov/table/ACSST1Y2023.S1601?q=Language%20Spoken%20at%20Home&g=040XX00US53.
4Cohen A, Rivara F, Marcuse E, McPhillips H, Davis R (2005, September). Are Language Barriers Associated With Serious Medical Events in Hospitalized Pediatric Patients?. Pediatrics, September 2005; 116 (3): 575–579. https://publications.aap.org/pediatrics/article-abstract/116/3/575/68390/Are-Language-Barriers-Associated-With-Serious?redirectedFrom=fulltext.
5Divi, et al (2007, April). Language proficiency and adverse events in US hospitals: a pilot study. International Journal for Quality in Health Care (2007, April). https://pubmed.ncbi.nlm.nih.gov/17277013/.
6Lion, et al (2013, July). Association Between Language, Serious Adverse Events, and Length of Stay Among Hospitalized Children. Hospital Pediatrics (2013, July). https://publications.aap.org/hospitalpediatrics/article-abstract/3/3/219/73365/Association-Between-Language-Serious-Adverse?redirectedFrom=fulltext?autologincheck=redirected.
7Gallagher R, Porter S, Monuteaux M, Stack A (2013, May). Unscheduled Return Visits to the Emergency Department: The Impact of Language. Pediatric Emergency Care 29(5):p 579-583. https://journals.lww.com/pec-online/abstract/2013/05000/unscheduled_return_visits_to_the_emergency.5.aspx.
8de Moissac D, Bowen S. Impact of Language Barriers on Quality of Care and Patient Safety for Official Language Minority Francophones in Canada. J Patient Exp. 2019 Mar;6(1):24-32. https://pubmed.ncbi.nlm.nih.gov/31236448/.
9Marshall E, Wong S, Haggerty J, Levesque JF (2010, February). Perceptions of unmet healthcare needs: what do Punjabi and Chinese-speaking immigrants think? A qualitative study. BMC Health Serv Res 10, 46 (2010). https://doi.org/10.1186/1472-6963-10-46.
10Pandey M, Maina RG, Amoyaw J, Li Y, Kamrul R, Michaels CR, Maroof R. Impacts of English language proficiency on healthcare access, use, and outcomes among immigrants: a qualitative study. BMC Health Serv Res. 2021 Jul 26;21(1):741. https://pmc.ncbi.nlm.nih.gov/articles/PMC8314461/#CR30.
11Oca S, Navas A, Leiman E, Buckland D (2021, July). Effect of language interpretation modality on throughput and mortality for critical care patients: A retrospective observational study. Journal of the American College of Emergeny Physicians Open. 2021 Jul 2;2(4):e12477. https://pmc.ncbi.nlm.nih.gov/articles/PMC8253091/#:~:text=The%20ICU%20mortality%20rate%20for,had%20in%E2%80%90person%20interpretation%20available.
12Rhee C, Jones TM, Hamad Y, et al (2019, February). Prevalence, Underlying Causes, and Preventability of Sepsis-Associated Mortality in US Acute Care Hospitals. JAMA Netw Open. 2019;2(2):e187571. doi:10.1001/jamanetworkopen.2018.7571. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2724768.
13 Liang L, Moore B, Soni A (2020, July). National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2017. Healthcare Cost & Utilization Project Statistical Brief #261. https://hcup-us.ahrq.gov/reports/statbriefs/sb261-Most-Expensive-Hospital-Conditions-2017.jsp.
14Newman-Toker DE, Wang Z, Zhu Y, et al (2020, May). Rate of diagnostic errors and serious misdiagnosis-related harms for major vascular events, infections, and cancers: Toward a national incidence estimate using the “Big Three.” Diagnosis (Berl) 2021; 8:67–84. https://pubmed.ncbi.nlm.nih.gov/32412440/.
14Centers for Disease Control and Prevention (2016, August). Making Healthcare Care Safer – Think Sepsis. https://www.cdc.gov/vitalsigns/pdf/2016-08-vitalsigns.pdf.


